The global arbitrage through migration can 10-20X A nurse’s earnings. In an era of universal labor mobility, few professions offer as dramatic an arbitrage opportunity as nursing. A profession that shows a labor shortage range of 16 to 50% in host countries. A registered nurse earning $300 a month in Kenya, Uzbekistan, or Vietnam can, within 12–36 months, step into a role in the United States or Saudi Arabia that pays $3,000 to $8,000 per month and, crucially, often includes free housing, flights, and health insurance. This is not a 2× or 3× salary increase. It is routinely 10× to 20×, sometimes more when housing, the single largest expense for any migrant, is covered.
When the multiplier reaches 10×, five years of overseas work equals fifty years of earnings at home. Seven years equals seventy. This is not incremental improvement but a transformational wealth creation compressed into a few years of a nurse’s career.
The Global Arbitrage That 10X Nurses’ Income
Take a typical example from the highest-return on Investment (ROI) cohort:
- Kenya public-sector nurse: ≈$400–$800 net per month.
- Same nurse in the United States (median RN salary 2025): ≈$7,800 gross → ≈$5,800–$6,200 take-home depending on state.
- Same nurse in Saudi Arabia (staff nurse, tax-free, with housing): 9,000–14,000 SAR ≈ $2,400–$3,730 net, plus zero rent, zero utilities, free flights home once a year.
Even the lower Saudi package is 6–9× the Kenyan salary before housing is factored in. Once housing is removed from expenses, which is easily $1,500–$2,500/month in any major US city and 4,000–8,000 SAR in Riyadh or Jeddah, the effective purchasing power and savings rate explode.
Real-world outcome reported by hundreds of nurses on forums, WhatsApp groups, and recruitment agencies:
- A Kenyan nurse in Saudi routinely saves $2,000–$3,000 every month.
- A Nigerian nurse in Texas or New York, after rent and taxes, still clears $3,500–$4,500 in savings and remittances.
- Five years at that rate = $120,000–$225,000 saved and sent home.
In Nairobi or Lagos, $200,000 buys multiple apartments or a small commercial building. In rural areas it buys land, a house, and funds university for an entire extended family. 5-7 years and the nurse returns as a millionaire in local terms.
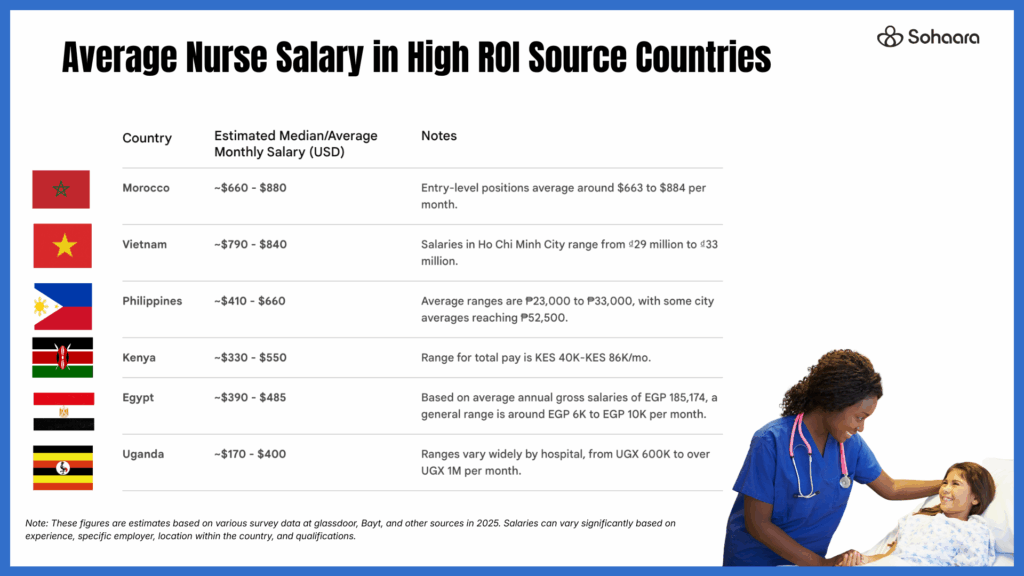
The Countries Where the Multiple is Highest
The arbitrage is not uniform; it is sharpest where local salaries collapsed or never rose with global standards:
- Kenya, Nigeria, Ghana, Uganda, Zimbabwe Multiplier: 12×–20× (US), 8×–15× (KSA with housing) English-speaking, large graduate output, relatively straightforward credential recognition.
- Central Asia (Uzbekistan, Kyrgyzstan, Tajikistan, Kazakhstan) Multiplier: 15×–25× low baseline salaries of $170–$650/month, nurses willing to learn English, almost no competition yet from large recruiters.
- Indonesia and Vietnam Multiplier: 12×–18× Huge graduate numbers, improving BSN programs, cultural adaptability, especially to Muslim-majority KSA for Indonesians.
- North Africa (Morocco, Tunisia, Egypt) Multiplier: 8×–15× Slightly higher local pay but still dramatic gaps, cultural continuity and existing Gulf migration corridors.
In every one of these countries, nursing salaries have not kept pace with inflation, currency devaluation, or global benchmarks, while the US and Saudi Arabia face structural shortages that will last decades. The US projects 200,000+ annual RN openings through 2033 and the Saudi Vision 2030 is adding entire new medical cities.
Why Housing is the Secret Multiplier
Rent is the silent killer of migrant dreams in most high-income countries. In the United States it routinely consumes 30–50% of a new immigrant nurse’s income in desirable states (California, New York, Texas metros).
Saudi Arabia flips the equation: virtually every hospital contract includes free, furnished, air-conditioned accommodation in secure compounds, often with pools, gyms, and transport to the hospital. A Filipino or Indian nurse who has worked both systems will tell you the same thing: “In America I earned more on paper, but in Saudi I saved more.”
Result: effective savings rate in Saudi frequently 70–90% of salary versus 30–50% in the US. A nurse earning “only” $3,000 net in Saudi with zero rent saves more per month than a nurse earning $6,000 in the US paying $2,000 rent plus utilities and transport.
Many nurses now strategically sequence the two destinations:
- Years 1–3 in Saudi Arabia: maximize savings, zero debt, build a financial runway.
- Then transition to the US easier once they have international experience, savings for exam fees, and a stronger résumé.
From Salary to Generational Wealth: Real Stories, Real Numbers
- Mercy, Kenyan nurse, 34 2019: earning KSh 45,000/month in Nairobi public hospital 2021–2025: staff nurse in Riyadh (11,500 SAR + housing) Saved $112,000 in four years, built a six-unit apartment block in Kisumu now generating KSh 240,000/month passive income, paid university fees for three siblings.
- Fatima, Uzbek nurse, 29 2023: 4 million UZS/month ($330) in Tashkent 2024–present: Texas hospital, EB-3 visa First year take-home after rent/taxes: $48,000 saved/remitted Bought two apartments in Tashkent outright; family now lives rent-free and collects second apartment’s rental income.
- Linh, Vietnamese nurse, 31 2022: ₫11 million/month in Ho Chi Minh City 2024–present: Jeddah private hospital, 10,500 SAR + full benefits Saving $2,800/month. Goal: $200,000 in five years to open a private clinic back in Đà Nẵng.
These are not outliers; they are the new normal in nursing WhatsApp groups from Lagos to Almaty.
The Financial Planning Revolution
A nurse who understands the arbitrage stops thinking in terms of “salary” and starts thinking in terms of compressed decades.
Simple planning framework now taught in pre-departure seminars:
- Year 0–1: Invest $2,000–$5,000 in NCLEX/SNLE preparation and recruitment (often financed by future earnings).
- Years 1–5: Save 60–85% of income ($2,000–$5,000/month).
- Return after 5–7 years: $150,000–$400,000.
- At home, that capital buys:
- Real estate generating 8–15% annual yield (apartments, shophouses, farmland).
- Businesses (clinics, pharmacies, schools).
- Full funding for children’s education, in country or abroad, if desired.
Risks and Mitigations
The possible risks associated with this migration and risk mitigation strategies, include:
- Exam failure: NCLEX pass rates for first-time international candidates now 55–70% with proper training and coaching.
- Recruitment scams: use only licensed agencies or direct hospital contracts.
- Family separation: mitigated by generous leave policies and, later, family reunification visas.
- Cultural adjustment and homesickness: compounds and diaspora communities help enormously).
- English proficiency and soft skills: Nurses who communicate proficiently in English and have leadership skills, double their salaries in 2 years rather than 4 years in KSA and get promotions faster in the US, which means up to 3x their initial salary.
Ethical Considerations and the Bigger Picture
Source countries lose talent, but they also gain remittances (Nigeria’s healthcare diaspora sent home $4–5 billion annually), knowledge transfer, and pressure to improve domestic conditions. The most forward-thinking governments (Philippines, Kenya, Indonesia) now treat nursing migration as a development strategy: train more than needed, export the surplus, import the capital and skills later.
Responsible recruiters and hospitals increasingly offer “circular migration” models: work abroad 5–7 years, return with savings and advanced certifications, teach or open private facilities. The nurse wins, the home country eventually wins, and destination countries fill critical gaps.
Conclusion: A Once-in-a-Generation Window
For a nurse in any of the high-ROI countries listed, the years 2025–2035 represent a historic convergence:
- Destination shortages deeper than ever.
- Streamlined licensing (NCLEX testing centers expanding, Saudi Dataflow faster).
- Digital preparation tools cheaper and more effective.
- Competition from recruiters still patchy outside Philippines/India.
Five years of disciplined work abroad can equal a lifetime career’s earning at home. Ten years can create dynastic wealth.
The nurse who boards that flight with an employment contract is not just changing jobs. She is stepping through a wormhole in personal economics, emerging on the other side with the financial life of someone who worked an entire lifetime, only she still has decades left to invest it, and pass it on.
For the ambitious, prepared nurse reading this in Nairobi, Tashkent, Jakarta, Marrakech, or Accra right now: the arbitrage is real, the path is clearer than ever, and the window, while wide open today, will not stay that way forever.
The question is no longer whether the opportunity exists. The only question is how quickly you will move to claim it.